
The eye is one of the most complex systems of the human body.1 Parts of the eye include, but are not limited to, the cornea, sclera, retina and optic nerve, which all work in conjunction with the brain to produce sight, arguably the most important sense (refer to figure 1).2 The cornea is the transparent outer layer of the front of the eye, which is continuous of the sclera, the tough outer coat of the eyeball.3 In a perfect eye, the cornea catches light rays and together with the lens, adjusts their focal length to allow the focal point to reach the retina at the back of the eye.4 The retina contains photoreceptor cells, which give an image colour before the optic nerve transfers the image as neural impulses to the brain for processing.5 Abnormalities in the shape of the cornea can cause the light rays to be focused in different directions on the retina, causing blurred vision.6 These refractive errors, also known as ametropic conditions, include myopia, hypermetropia, astigmatism and presbyopia.7

MYOPIA
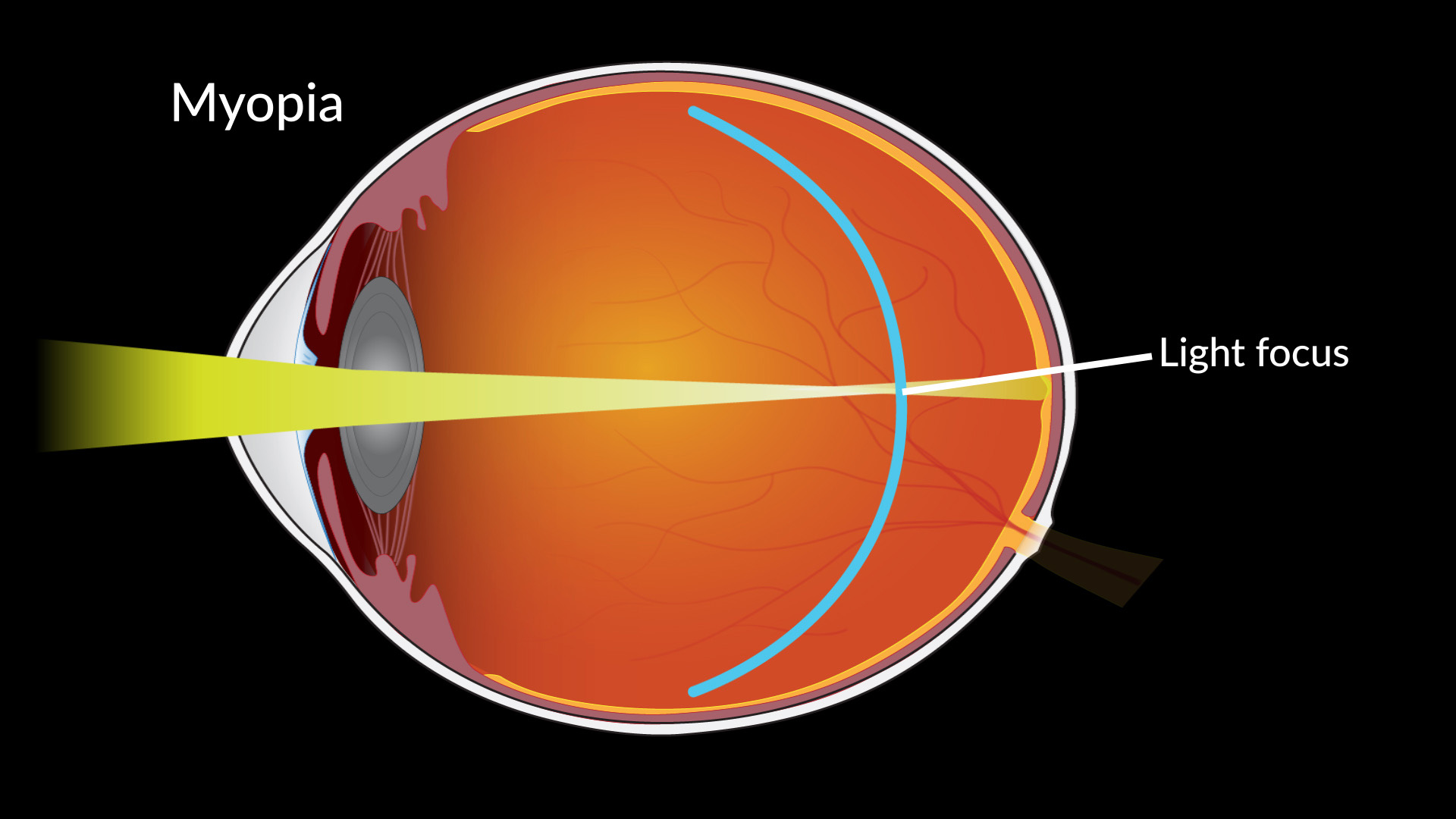
Myopia or nearsightedness occurs when the eyeball is too long (indicated by a longer axial diametre) for the refractive power of the cornea and lens.9 As the cornea and lens move further away form the retina, the further the focal point is positioned in front of the retina, increasing distant blurred vision.10 This is corrected with a concave lens or by flattening the surface of the cornea to reduce the axial diameter.11 Twin studies show inheritability of refractive errors; ethnicity, genetics and age are the main factors causing myopia however our lifestyles such as increased use of hand held devices, poor diets high in processed sugar rich foods and high academic demands are also a likely cause.12 Higher levels of education show higher rates of myopia, indicating a link between education demands and myopia.13 Myopia has significant health consequences including financial, psychological, quality of life, and indirect risks of eventual blindness from ocular disease.14
Onset of myopia is most common in childhood at approximate age of six years and is now in epidemic proportions.15 In developed countries, myopia rates have increased over the last few decades.16 The population rate of myopia is approximately 25% in the USA to as much as 90% in some parts of China.17 Twenty percent of Australian children suffer from myopia, a concerning statistic considering there is a significant link between ocular diseases and myopia.18 Myopia has also been associated with glaucoma and cataracts. Glaucoma is an ocular disease that damages the optic nerve through the build up of fluid and therefore pressure in the front of the eye.19 Damage to the optic nerve results in gradual or instantaneous vision loss, making glaucoma a blinding disease.20 As the severity of myopia or the axial diametre increases, so does the risk factor for glaucoma.21 There is a higher risk of developing glaucoma from myopia, compared with heart disease from smoking.22 An estimated 300,000 Australians have glaucoma, majority of which could have been prevented by regular ocular checks for myopia.23
The most common form of ametropic (including myopia) correction worldwide is prescription glasses.24 Eighty-seven percent of people utilise glasses, followed by soft contact lenses.25 However, unlike these methods, orthokeratology can slow the progression of childhood myopia by up to 80% and thus reduce the risk of glaucoma.26
ORTHOKERATOLOGY
Orthokeratology or Corneal Refractive Therapy (CRT) refers to the use of hard gas-permeable contact lenses called Ortho-K, which temporarily remodel the surface of the cornea to reduce or eliminate refractive error.27 The origins of Orthokeratology are associated with the ancient Chinese, who slept with small sand-filled teabags on their eyelids to correct their unaided vision.28
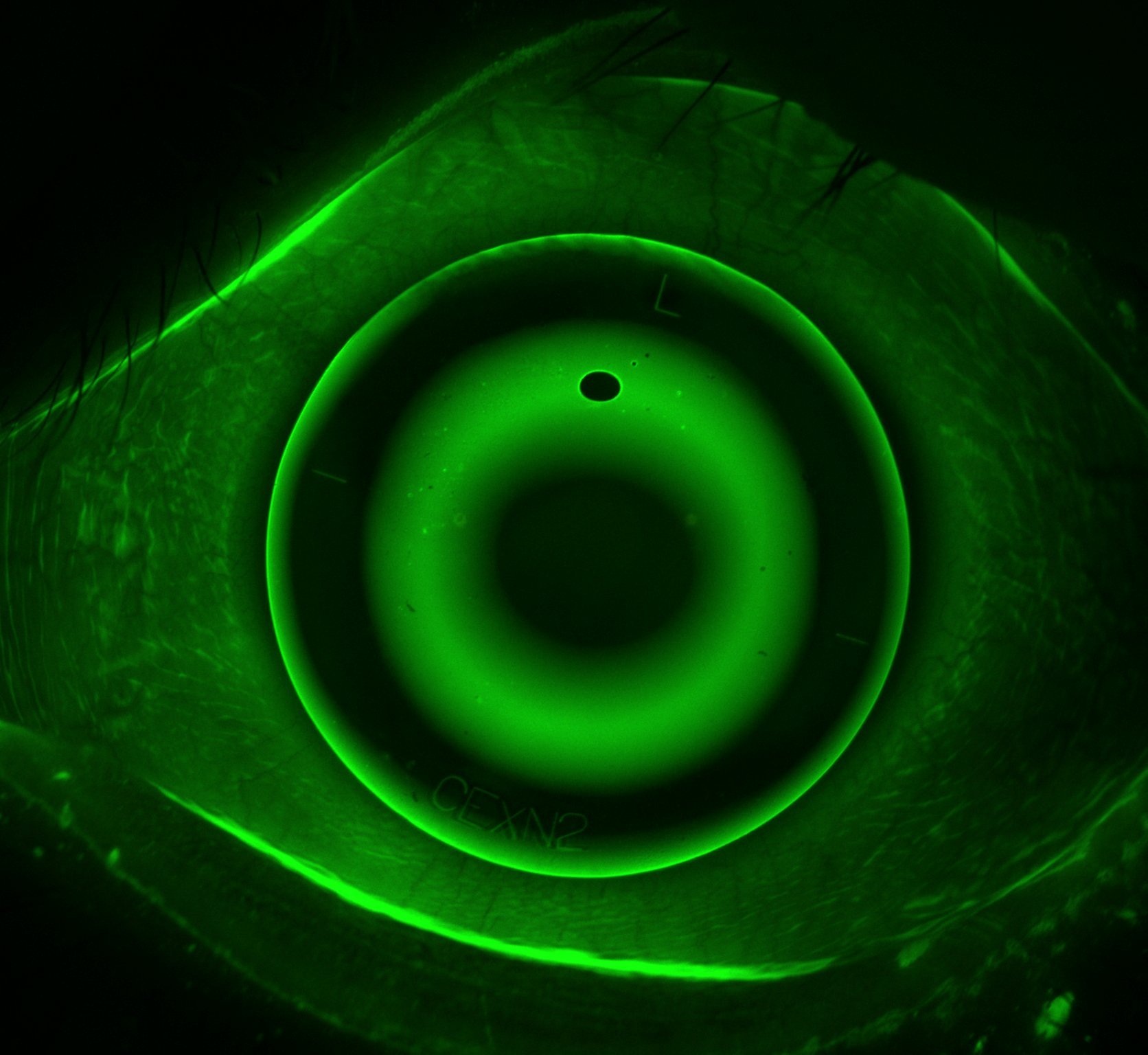
Ortho-K Lenses are worn at night while sleeping to mould the surface of the cornea.29 Most lenses are 0.2mm thick or less and have a special curve structure.30 When worn, the base curve pushes down on the centre of the cornea, therefore flattening it and correcting myopia.31 The shape of the lens and therefore correction is specific to the severity of the ametropia of the patient (refer to figure 2).32 Ortho-K Lenses are specially designed for each individual, shaped in such a way to either flatten the cornea, steepen the cornea or to simply mould the surface into the perfect shape eliminating abnormalities.33 The lenses improve unaided vision during the day, by approximately 50-75% during the first night and near total correction within one week to ten days.34

Correct fitting, follow up and care of the Ortho-K lenses is paramount to the success of CR.36 In order to understand this, it is first necessary to understand how the lenses work with the biomechanics of the human eye.37 The plastic of the lens obtains large amounts of silicone a hydrophobic molecule, meaning it repels water.38 By repelling water the eye becomes very dry making the lens uncomfortable to wear jeopardising correction. A contact lens needs to be hydrophilic (attract water) to work with the biomechanics of the eye.39 Ortho-K Lenses are hydrophilic because a deep protein removal agent such as Progent or Medicon used once a month can rotate the molecules within.40 It mixes two solutions, sodium hypochlorite and potassium bromide, which make a potent cleaner but also cause the surface molecule of the silicone to spin.41 The lenses also require daily cleaning with multipurpose solution such as Menicare.42 This step removes the material deposits on the lens during wear.43 Secondly, disinfecting and storing the lenses in fresh solution in a specialised lens case upholds its condition by ensuring the lens is completely submerged.44
The process of fitting Ortho-K involves two very important factors: an eye health check and corneal topography.45 Corneal topography is the detailed mapping or charting of the features of the cornea, used in conjunction with computer software to produce a curvature map.46 Early topography includes Placido’s disc first noted in the late 19th century, based on the principle of assessing the reflection of a concentric set of white rings from the convex anterior surface of the cornea (refer to figure 3).47 Computerised topography is colour coded to show the elevation in the cornea: any point on the cornea that is higher than the best-fit sphere will be shown as a peak – in ‘hotter’ colours such as orange, red and white.48 Any point that is lower will be shown as a valley – in ‘cooler’ colours such as blue, azure and black.49 Green and yellow represent areas of best-fit sphere.50 Curvature maps are essential in the design of Ortho-K Lenses and are used to illustrate the change in curvature of the cornea during CRT.51

Curvature maps and axial diameter measurements work in conjunction with computer software such as EyeSpace, to design the lenses (refer to figure 4).53 The lenses are designed based on the patients’ axial diameter, ocular condition and prescription lens.54 This step is important because if the Ortho-K Lenses does not fit properly then correction of the Myopia is not made and in turn further eye damage from ocular disease is probable later in life.55 Once designed, the lenses are manufactured on a computer-assisted lathe.56 By understanding the colour system of corneal topography the Orthokeratologist is able to read the fit of the lens and access the correction level of the ametropic condition.57 They can therefore alter the lens fit if required by making a new lens.58 By perfecting fit, the best possible correction can be made to halt myopic progression.59

Correct cleaning prevents the major disadvantage of contact lenses, which is a bacterial infection of the cornea called Microbial Keratitis.61 This same risk applies to all contact lenses.62 Another risk includes trauma while inserting a lens such as scratching the cornea.63 However, with specialised training this rarely occurs.64 A lens can also be fitted that produces a result which isn’t visually desirable, however just like wearing a pair of glasses they can be adjusted.65 The last disadvantage is that not everyone is a candidate for CRT.66 An eye examination by an orthokeratologist determines whether a person is a candidate for Ortho-K.67 Generally, anyone who has -8 dioptres or above myopia is not a candidate because their cornea would have to be flattened to an impossible amount.68
Benefits of Ortho-K Lenses include providing clear unassisted vision during the day, which prevents dry eyes and improves comfort.69 It also eliminates the need for prescription glasses and the risk of the lenses falling out.70 Orthokeratology is also non-invasive and completely reversible unlike laser surgery (LASIK).71 There are also benefits for children as the lenses are worn at home under direct supervision, therefore the lens cannot be lost at school.72 Orthokeratology is superior to other ametropic treatments as it prevents childhood myopia, by reducing the axial length of the eyeball and correcting the refractive error.73
CASE STUDY: SUBJECT A
Before CRT Condition: severe myopia - left eye 6/100 (-6.25 dioptres) Age: seventeen years old (diagnosed at six) Symptoms: headache, dizziness, blurred near vision, mild optic nerve damage.
The patient was followed through Corneal Refractive Therapy for two months to determine the effectiveness of treatment.74 Topography of Subject A’s first visit (refer to figure 5A) initial left cornea indicates severe myopia shown by the warm colours in the centre of the cornea which represent steeper areas than the best-fit sphere or peak.75 Topography of Subject A’s second visit after treatment of left cornea after two months of Ortho-K use (refer to figure 5B) indicates the flattening of the centre of the cornea shown by cool colours such as the blue representing areas flatter than the best-fit sphere or valley.76 A comparison topography map of pretreatment and post treatment (refer to figure 5C) highlights the large change (flattening) in the cornea curvature, illustrated using a dark blue circle. The large dark blue circle is also referred to as a perfect result.77
Two months into CRT Condition: better than perfect vision, myopia progression halted - left eye 6/6 (+0.50) Age: seventeen years old Symptoms: all corrected even the mild optic nerve damage.

Orthokeratology (CRT) was successful in Subject A’s topographies as the Ortho-K Lens was able to flatten Subject A’s cornea significantly correcting the patient’s myopia. This patient will not only reap the short-term benefits of the Ortho-K Lenses such as convenience, ability to provide unaided vision during the day and reversibility so laser surgery can be explored later if desired, but also the long-term benefits including indirectly reducing their risk of ocular disease in later life such as glaucoma.
CONCLUSION
The eye is the body’s organ of sight and any ametropic conditions of the eye such as myopia linked to ocular disease should be treated aggressively to prevent blindness.79 Myopia is at epidemic proportions, with 22.9% of the world’s population affected.80 Severe myopia dramatically increases the likelihood of developing glaucoma, macular degeneration, cataracts or retinal detachment.81 Orthokeratology works to temporarily remodel the surface of the cornea to reduce or eliminate ametropia.82 Orthokeratology also slows and even halts the progression of childhood myopia by preventing the axial diameter of the eye from increasing.83 Using Orthokeratology as a first resort over prescription glasses may reduce the severity of childhood myopia, and hence decrease the risk of glaucoma in later life.84 Orthokeratology does slow the progression of childhood myopia, thus it is plausible to suggest that to a significant extent, it can indirectly reduce the rate of glaucoma.85 As the risk of glaucoma increases with untreated myopia, and with 22.9% of the world’s population suffering from myopia, the prospects for Orthokeratology are endless.86
References
- Taylor, T. ‘Eye’, [website], (1999) http://www.innerbody.com/image_nervov/nerv06-new.html accessed 10 Apr. 2017
- Segre, L. ‘Eye Anatomy: Parts Of The Eye, All About Vision’ [website], (2016) http://www.allaboutvision.com/resources/anatomy.htm accessed 11 Apr. 2017
- Roberts, A. Human Anatomy The Definitive Visual Guide, p125, (2016) DK London
- National Keratoconus Foundation, ‘How Does The Human Eye Work?’ [website], (2016) https://www.nkcf.org/about-keratoconus/how-the-human-eye-works/ accessed 6 Apr. 2017
- Hubel, D.H. Eye, Brain and Vision (Henry Holt an Company, 1995), Issue 22 of Scientific American Library Series, chap. 3
- Deepinder, D.K. ‘Refractive Disorders’ [website], (2016), http://www.msdmanuals.com/en-au/home/eye-disorders/refractive-disorders/refractive-disorders#resourcesInArticle accessed 11 Apr. 2017
- Fulton, J.T. ‘Myopia & Ametropia as Complex Syndromes’ [website], (2009) http://neuronresearch.net/vision/clinical/myopia.htm accessed 11 Apr. 2017
- Roberts, A. Human Anatomy The Definitive Visual Guide, [image] p125, (2016) DK London
- National Eye Institute, ‘Facts about Myopia’, [website], (2016) https://nei.nih.gov/health/errors/myopia accessed 15 Apr. 2017
- Lowth, M. ‘Short Sight Myopia’, [website], (2016) https://patient.info/health/short-sight- accessed 15 Apr. 2017
- Simanek, D. ‘Lens Basics’, [website], (2014) https://www.lhup.edu/~dsimanek/scenario/lenses.htm accessed 20 Apr.2017
- Morgan, P.B., Woods, C.A., Efron N, et al. ‘International Contact Lens Prescribing in 2016’ [website], (2017) http://www.clspectrum.com/issues/2017/january/international-contact-lens-prescribing-in-2016#table-2 accessed 15 Apr. 2017
- Wensor, M., McCarty C.A. & Taylor H.R. ‘Prevalence and Risk Factors of Myopia in Victoria, Australia’, [website], (1999) http://jamanetwork.com/journals/jamaophthalmology/fullarticle/411882 accessed 9 Apr. 2017
- Grigg, J., Jamieson, R. ‘Socioeconomic impact of low vision and blindness from paediatric eye disease in Australia, [website], (2016) http://www.savesightinstitute.org.au/wp-content/uploads/2016/09/Open-Eyes-Report-into-Paediatric-Eye-Disease-in-Australia-July-2016.pdf accessed 20 Apr. 2017
- Dolgin, E. ‘The Myopia Boom’, [website], (2015) http://www.nature.com/news/the-myopia-boom-1.17120 accessed 30 Apr. 2017
- Seet, B., Wong, T.Y., Tan, D. et al, ‘Myopia in Singapore: taking a public approach’, [website], (2012) http://bjo.bmj.com/content/85/5/521 accessed 30 Apr. 2017
- Lin L.K, Shih Y.F, Lee Y.C, et al. ‘Changes in Ocular Refraction and Its Components Among Medical Students: A 5-Year Longitudinal Study,’ Optometry and Vision Science, 73, (1996), pp495–498
- Kelly, G. ‘Interview with Lachlan Scott-Hoy’ [personal communication], 16 March 2017
- Boyd, K. ‘What is Glaucoma’, [website], (2017) https://www.aao.org/eye-health/diseases/what-is-glaucoma accessed 10 Apr. 2017
- Lin, A.S.M, Constable, I.J. ‘Colour Atlas of Ophthalmology’, PG Medical Books, Singapore (1982)
- Marcus, M.W., de Vries, M.M., Junoy Montolio, F.G, et al. ‘Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis’, [website], (2011) https://www.ncbi.nlm.nih.gov/pubmed/21684603 accessed 15 Apr. 2017
- Flitcroft, D. ‘The complex interactions of retinal, optical and environmental factors in myopia aetiology’, (2012) Children’s University Hospital, Temple Street, Dublin, Ireland
- Young, T. ‘A review: the association between Myopia and Glaucoma’, [website], (2017) https://www.ophth.wisc.edu/the-association-between-myopia-and-glaucoma/ accessed 31 Apr. 2017
- Schiefer, U., Kraus, C., Baumbach, P. et al, ‘Refractive Errors’, [website], (2016) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5143802/ accessed 9 Apr. 2017
- Kelly, G. ‘Orthokeratology Survey’ [SurveyMonkey], 28 February 2017
- Smith, M.J. & Walline, J.J. ‘Controlling myopia progression in children and adolescents’, [website], (2015) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4542412/ accessed 9 Apr. 2017
- Downie, L. ‘Orthokeratology: a clinical review – part one’, CET Orthokeratology, (2015) pg. 44-48.
- Tompkins, J. ‘Vision Quest’, Los Angeles Magazine, Health, Jan. 2004, pg. 50 https://books.google.com.au/books?id=210EAAAAMBAJ&pg=PA46&lpg=PA46&dq=sandbags+on+eyelids+ancient+china&source=bl&ots=n1FReKDzQF&sig=1OXsBZhmnhehou7py1yZXSxnF7o&hl=en&sa=X&ved=0ahUKEwizyt69p7LTAhWFVrwKHUa7DuUQ6AEIJjAB#v=onepage&q&f=false accessed 20 Apr. 2017
- Innovative Eye Care, ‘Orthokeratology’, [website], (2016) http://innovativeeyecare.com.au/what-we-do/orthokeratology accessed 15 Apr. 2017
- West End Eye Care, ‘Ortho-K Sleep Wake See’, [website], (2015) http://eyecarepaducah.com/ortho-k/ accessed 15 Apr. 2017
- Lowth, M., Tidy, C. ‘Refraction and Refractive Errors’, [website], (2016) https://patient.info/doctor/refraction-and-refractive-errors accessed 12 Apr. 2017
- Heiting, G. ‘OrthoK And Corneal Refractive Therapy: Overnight Contacts To Correct Myopia’ [website], (2016) http://www.allaboutvision.com/contacts/orthok.htm accessed 1 Apr. 2017
- Fung, M. ‘Configuration of the Ortho-K Lens’, [image], (2016) http://emedicine.medscape.com/article/1196836-overview?pa=6AzZxAWCxvULX%2FRa8x46d%2BcTl9g9nzHNDUM9dqxarywOpxp%2BhOwkyQ9q%2FvyXnJQNZj62Mgfkyex%2B12xIXlGUjA2R7IblBRA7%2BfuIyyrgIPE%3D#a3
- Daniels, K. ‘Consider OrthoK For Myopia Control’ [website], (2012) https://www.reviewofoptometry.com/article/consider-ortho-k-for-myopia-control accessed June 2. 2017
- Yue, L., Pelying, X. ‘The Safety of Orthokeratology: A Systematic Review’, [website], (2016) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4697954/ accessed 11 Apr. 2017
- Owen, M.J. ‘Silicone Hydrophobicity and Oleophilicity’, [website], (2004) https://link.springer.com/article/10.1007/s12633-014-9188-0 accessed 11 Apr. 2017
- Edrington, T. ‘Irregular Corneas: Diagnosis and Management’, [website], (2014), Southern Californian College of Optometry http://www.aaopt.org/sites/default/files/userfiles/2014_Handouts/DPCL.pdf accessed 15 Apr. 2017
- Shady Grove Eye and Vision Care, ‘Caring For Your Ortho-K Lenses’, [website], (2016) https://www.youreyesite.com/eye-care-information/caring-ortho-k-lenses/ accessed 9 Apr. 2017
- Menicon, ‘Eye Health, Handling and Care’, (2017) http://www.menicon.com/consumer/ accessed May 1. 2017
- Menicon, ‘Menicon Z Night’ [website], (2017) http://www.menicon.co.uk/pro/our-products/gp-lens/menicon-z-night/ accessed 11 Apr. 2017
- Innovative eye care, ‘Care of Orthokeratology Lenses’, [wesite], (2016) https://www.innovativeeyecare.com.au/patient-resources/care-of-orthokeratology-lenses accessed May 1. 2017
- Herzberg, C. ‘An Update on Orthokeratology’, [website], (2010), https://www.clspectrum.com/issues/2010/march-2010/an-update-on-orthokeratology accessed May 2. 2017
- Gupta, R. ‘Corneal Topography’, [PowerPoint], (2015) https://www.slideshare.net/RamanGupta4/corneal-topographyraman?next_slideshow=1 accessed 5 Apr. 2017
- Fung, M.W. ‘Corneal Topography and Imaging’, [website], (2016) http://emedicine.medscape.com/article/1196836-overview?pa=6AzZxAWCxvULX%2FRa8x46d%2BcTl9g9nzHNDUM9dqxarywOpxp%2BhOwkyQ9q%2FvyXnJQNZj62Mgfkyex%2B12xIXlGUjA2R7IblBRA7%2BfuIyyrgIPE%3D#a3 accessed 7 Apr. 2017
- Greenwald, M.F., Vislisel J.M. & Greiner, M.A. ‘Corneal Imaging: An Introduction’, [website], (2016) http://webeye.ophth.uiowa.edu/eyeforum/tutorials/Corneal-Imaging/Index.htm accessed 7 Apr. 2017
- eJournal of Ophthalmology, ‘Topographic Displays – Elevation Based Devices’, [website], (2011) http://www.ejournalofophthalmology.com/ejo/ejo27c.html accessed 14 Apr. 2017
- Anderson, D. ‘Understanding Corneal Topography’, [website], (2016) http://www..aoa.org/Documents/optometric-staff/Articles/Understanding-Corneal-Topography.pdf accessed 5 Apr. 2017
- Kopp, K. ‘Review of Corneal Reshaping: Orthokeratology, [website], (2017), https://www.mivision.com.au/review-of-corneal-reshaping-orthokeratology/ accessed 11 Apr. 2017
- Eye Wiki, ‘Corneal topography’, [image], American Academy of Ophthalmology, (2015) http://eyewiki.org/testwiki/index.php?title=Corneal_topography
- Brown, J. ‘EyeSpace Manual Documentation’, [website], (2014) https://media.readthedocs.org/pdf/eyespace-docs/latest/eyespace-docs.pdf accessed May 2. 2017
- E&E Optics, ‘Ortho K Lens – trouble shoot’, [website], (2015) http://eandeopticsusa.com/ortho-K-lens/ortho-k-troubleshoot/?view=mobile accessed 14 Apr. 2017
- Scope Texas Eye Consultants, ‘Ortho K and Kids’, [website], (2016) http://www.scopevisioncare.com/en/ortho-k/ accessed 1 May 2017
- E&E Optics, ‘Lenses for Ortho-K’, [website], (2015) http://eandeopticsusa.com/home/who-we-are/?view=mobile accessed 14 Apr. 2017
- Watkins, A. ‘Corneal Topography’, [website], (2016), http://www.andrewwatkins.com.au/topography.php accessed 29 Apr. 2017
- RJK Optometry, ‘Orthokeratology’, [website], (2017) http://rjkoptometry.com.au/professional-eyecare/ortho-keratology/ accessed 18 May 2017
- Innovative Eye Care, Subject A’s Lens Design [image] 5 November 2013
- Turbert, D. ‘What is Bacterial Keratitis, [website], (2017) http://www.aao.org/eye-health/diseases/what-is-bacterial-keratitis accessed 29 May 2017
- Garg, A. ‘Ocular Trauma: Acute Evaluation, Cataract, Glaucoma’, [website], (2015) http://www.eyewiki.aao.org/Ocular_Trauma%3A_Acute_Evaluation,_Cataract,_Glaucoma accessed 20 Apr. 2017
- My Alcon, ‘Contact Lens Insertion and Removal Video’[website], (2016) https://www.myalcon.com/tools-resources/patient-education/contracts-insertion-and-removal-training.shtml accessed 12 Apr. 2017
- Santini, B. ‘All About That Base Curve’, [website], (2017) http://www.2020mag.com/article/all-about-that-base-curve accesse

Related blogs
Browse through our selection of related blogs to deepen your understanding and discover more on similar topics.
Orthokeratology (Ortho-K Night Lenses) | Innovative Eye Care | Adelaide Clinic

Myopia Control & Management | Innovative Eye Care | Adelaide Clinic

Dry Eyes Guide | Causes, Symptoms & Treatment | Innovative Eye Care Adelaide

Eye Health Hub | Keratoconus, Myopia, Dry Eye & Red Eye Care | Innovative Eye Care Adelaide


%20(1).png)


Dry or watery eyes? The solution may be a plumbing job

Colour vision deficiencies

Vision training: there's more than meets the eye!


Dry eye disease and the DEWS II

Blepharitis and dry eye, chicken or the egg?


Visual Snow

The Link Between Healthy Eating and Healthy Eyes

Headaches, Eye-Aches and Vision Changes

Helpful or hype? Blue light filters

Allergy Eye

How Do I Know If I Want A Multicoat?

Computer Vision Syndrome and Working from Home


Things All Contact Lens Wearers Should Know

Why can't I use tap water with my contact lenses?

